

















Beauty News, Guide & Information, Skin Conditions, Vivo Red Light
Red Light Therapy Questions Part 1: Devices, Wavelengths and Infrared Light Explained

Jul
Red light therapy (PBM) tends to raise the same questions time and again. That is why we are dedicating this series to the topics we hear about most. In this first part, we cover red light therapy devices, whether more wavelengths are actually better, why some LEDs appear to not be working, and the difference between red light therapy and other forms of infrared light.
We also look at the differences between Vivo models. If your question is not covered here, visit our full FAQ page for more information.
Questions About Devices and Technology
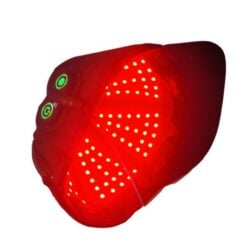
It looks like some of the lights are not on. Is that normal?
The short answer: yes, completely normal. Near-infrared LEDs are barely visible because near-infrared light falls outside the visible spectrum. Wavelengths like 810, 830, 850 and 1060 nm are virtually invisible to the naked eye, even though they are working perfectly.
Our panels combine visible red light with near-infrared light (NIR). The human eye perceives light in roughly the 380 to 780 nanometer (nm) range. Red light sits around 620 to 750 nm and is clearly visible. Near-infrared starts just above that range and is almost entirely invisible to us.
Depending on the model, Vivo panels use visible red wavelengths such as 630 nm, 660 nm and 670 nm, alongside near-infrared wavelengths such as 810 nm, 830 nm, 850 nm and, in some models, 1060 nm. This is why the red LEDs glow visibly while the NIR LEDs appear dim or even completely off, despite being fully active.
A simple way to think about it: a classic TV remote uses invisible near-infrared light around 940 nm. You cannot see it, but the signal is there and works just fine. The near-infrared LEDs in a red light panel work in exactly the same way. Invisible does not mean absent.
Red light is primarily associated with more superficial applications, while near-infrared penetrates deeper into tissue. That said, there is significant overlap in how they work, which is precisely why the two are so often combined in a single panel.
How deeply the light penetrates depends on a number of factors, including wavelength, light intensity, distance from the body, and the type of tissue being treated.
In a darkened room, you may notice a faint reddish or purple glow from the NIR LEDs. A phone camera can often detect near-infrared more clearly than the naked eye, though this varies by device, making it a useful way to check whether your NIR LEDs are active.

Are more wavelengths better?
The short answer: not automatically. What matters is not the number of wavelengths but the right wavelengths, delivered at sufficient strength and with the correct dosage.
In red light therapy, also known as photobiomodulation (PBM), wavelengths are the foundation of how the therapy works. A wavelength is essentially the “colour” of the light. It determines not only how deeply the light can penetrate tissue, but also which processes in and around the cell are influenced.
Red wavelengths around 630 to 680 nm are often associated in PBM research with cytochrome c oxidase (CCO), an enzyme in the mitochondria involved in cellular energy processes. Near-infrared in the range of roughly 800 to 1100 nm is more commonly linked to deeper tissue penetration and additional mechanisms, including its influence on water molecules in and around cells.
None of that means more wavelengths automatically leads to better results. In practice, what counts is a considered selection of active wavelengths present at sufficient strength. Packing too many different wavelengths into one panel risks spreading the light output too thin, reducing the effective dose at each relevant wavelength.
Think of it like a smoothie: a few well-chosen ingredients can work beautifully together, but add too many and the balance gets lost.
A smart combination of a limited number of well-researched wavelengths is therefore often more effective than a panel that looks impressive on paper but delivers too little at each individual wavelength.
International guidelines, including those from WALT (World Association for Photobiomodulation Therapy), also emphasise that the effectiveness of red light therapy depends on multiple factors, not wavelength alone, but also light intensity, dosage and treatment time. As their guidance notes, both too little and too much light can reduce results.
In short: do not just look at how many wavelengths a panel offers. Focus on which wavelengths they are, how strong they are, and what the right dosage is for your specific application.

This chart shows that the most established PBM wavelengths are centred around 633 nm, 660 nm, 808/810 nm and 830 nm.
Additional wavelengths such as 670 nm and 1064 nm are genuinely interesting additions, but they are not a prerequisite for a panel to be effective or to penetrate deeply.
What is the difference between the BioPhoton 3.0 and the BioPhoton+?
The short answer: the BioPhoton 3.0 is the lighter, gentler all-rounder; the BioPhoton+ is the more powerful version designed for shorter treatment times. Both offer the same hybrid approach: usable at a distance and safely directly on the skin, with no fan noise.
Both models use the same five red and near-infrared wavelengths and are passively cooled, meaning no fan, no disruptive noise, and a quieter, more relaxed treatment experience with virtually no measurable EMF.
The main difference lies in power output and build. The BioPhoton 3.0 is the lighter, gentler model. It is easy to position and well suited to a calm, controlled approach to dosing, making it an accessible all-round choice for many people, including those who prefer a softer treatment.
The BioPhoton+ is the more powerful and robust option. Its higher light output means shorter treatment times are generally sufficient, making it particularly appealing for those who want to treat more efficiently or are looking for a more professional-grade device.

Is red light therapy the same as an infrared sauna or a heat lamp?
The short answer: no. An infrared sauna or heat lamp works primarily through warmth, while red light therapy works through specific wavelengths of light that support cellular processes.
These terms are often used interchangeably online, but they are not the same thing. An infrared sauna typically uses far infrared (FIR), roughly from 3000 nm upwards, and is primarily designed to heat the body. The effect is therefore mainly thermal: warmth, sweating, relaxation and improved circulation.
Red light therapy, or photobiomodulation (PBM), works differently. The focus is not heat but specific photons from red and near-infrared light, broadly in the 630 to 1100 nm range, that can influence biological processes in the tissue. PBM is described in the scientific literature as a non-thermal light application. It is still regularly referred to by researchers as LLLT (low-level laser therapy) or cold laser therapy, even though a device may feel pleasantly warm in practice, similar to gentle spring sunshine.
That does not mean one is better than the other. They simply serve different purposes. Heat can be genuinely beneficial for relaxation, circulation and muscle tension. PBM is primarily discussed in the context of supporting recovery, pain modulation and inflammation regulation, without heat being the primary mechanism.
Eye safety is also worth distinguishing here. An infrared sauna or heat lamp is not designed to look into, and prolonged or intense infrared exposure can cause eye damage, including to the lens. PBM for the eyes is an entirely separate area of research, with red and near-infrared light showing promising results in some studies for eye health, including retinal and macular conditions.
The two can be used alongside each other, though it is worth keeping them in separate sessions if your goal is to maximise the light-based effects of PBM. There is evidence to suggest that skin temperature can influence how light disperses through tissue, with cooler skin potentially allowing for slightly deeper penetration. For that reason, combining red light therapy with intense heat sources like a sauna or heat lamp in the same session may not be ideal.
In short: an infrared sauna or heat lamp works primarily through warmth. Red light therapy uses specific wavelengths of light to support biological processes in the body, without heat being the primary goal. They are frequently confused, but they are not the same thing, and they tend to be most valuable for different purposes.






















 Beauty Products
Beauty Products By Skintype
By Skintype Brands A-Z
Brands A-Z Wellness
Wellness Health / Nutrition
Health / Nutrition